| Clinical findings | Mostly asymptomatic slow-growing, mobile, non-sensitive mass; Symptoms by compression of adjacent structures; Location: thigh, interscapular, mediastinum, back, head-and neck; Peak incidence: 30 - 50 years, female > male; DD liposarcoma, lipoma, angiolipoma |
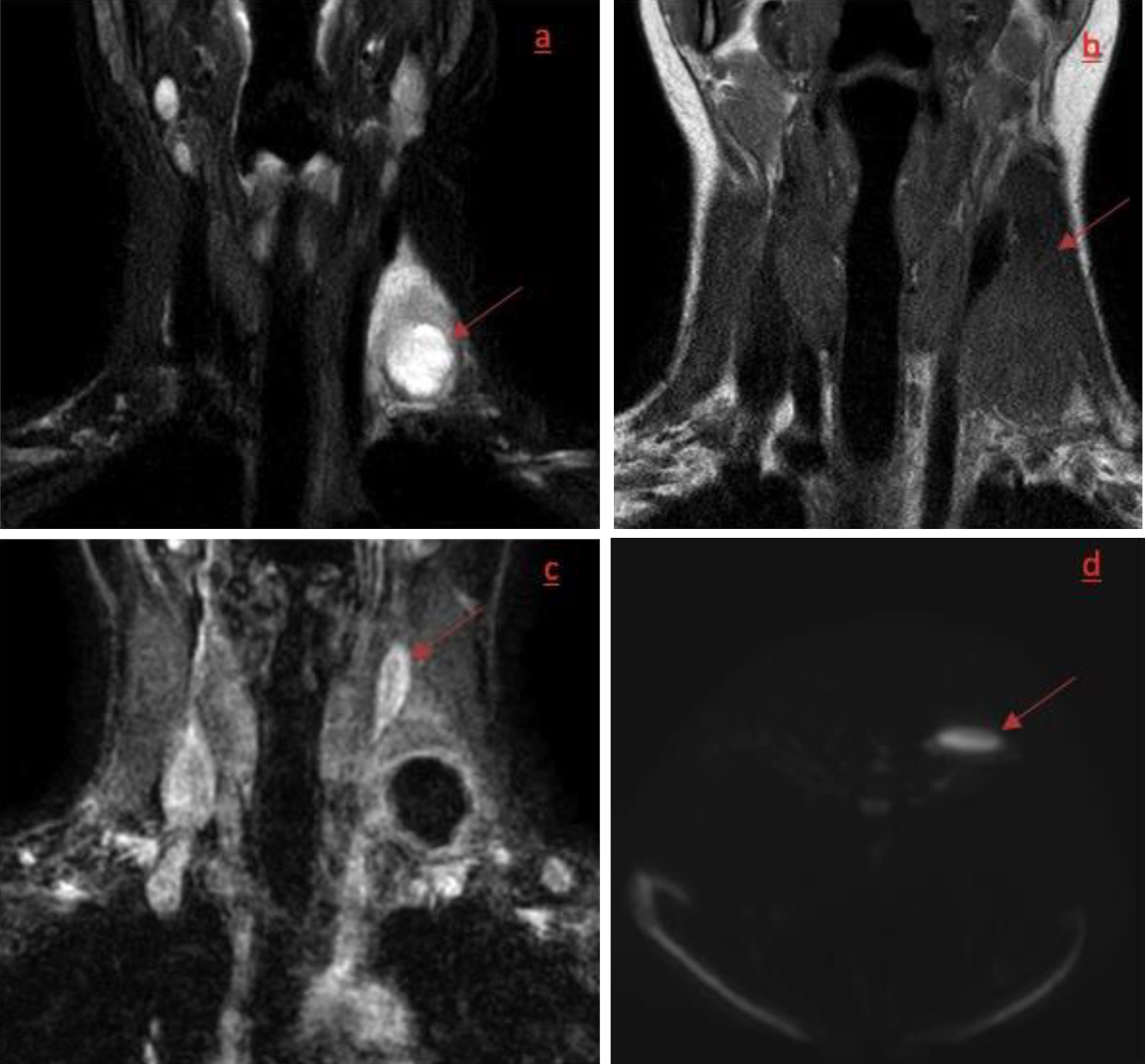
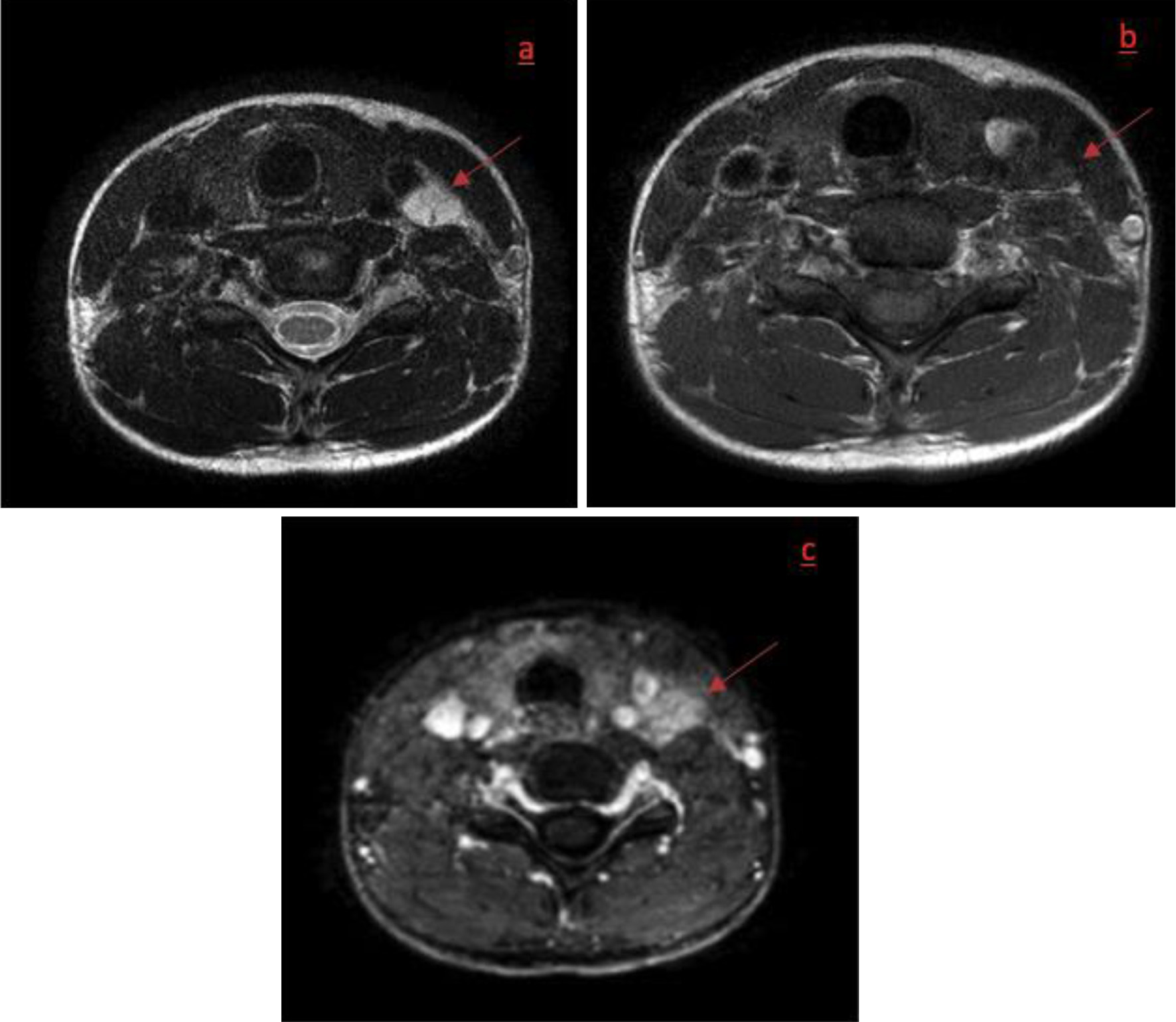
| Imaging [9] | Ultrasonography: hyperechogenic mass with hypervascularity +/- arteriovenous shunts; MRI: imaging of choice: 1) Well-delineated mass, vascularized, enhancing after contrast injection; 2) T1/T2: high signal intensity but less than subcutaneous fat; 3) Fat saturation sequences: no removing signal; CT with contrast: hypervascularity and septae; Non-contrast CT: hypodense and well-delineate; difficult to distinguish from subcutaneous adipose tissue; PET: high metabolic activity - obsolete |
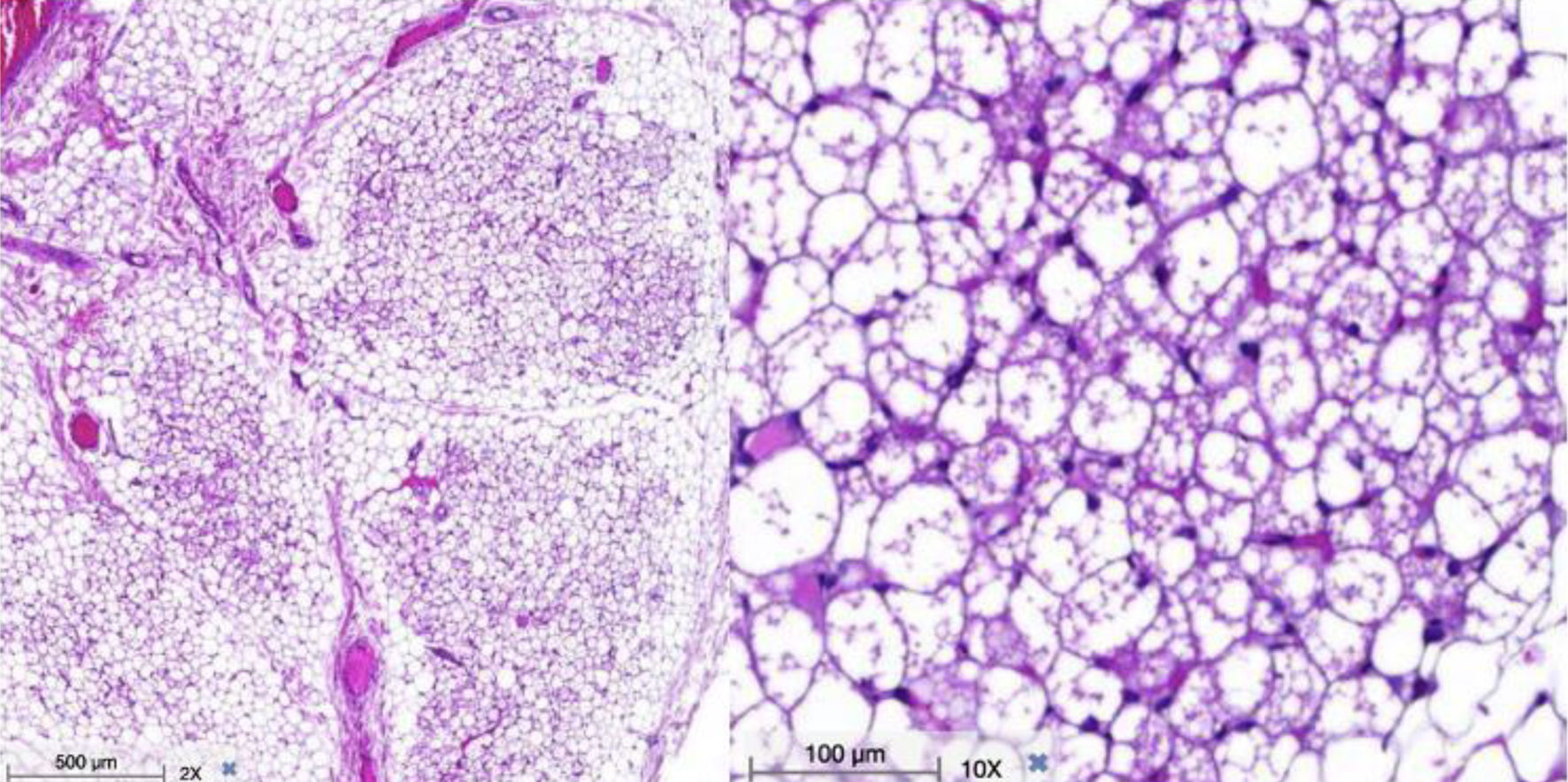
| Histology | Macroscopic: soft rubbery mass; Microscopic: 1) Multivacuolated brown adipocytes; 2) Small round central nucleus with large amount of eosinophilic cytoplasm; 3) Multiple small vacuoles; 4) Four subtypes: typical, spindle, lipoma-like and myxoid |
| Treatment | Surgical excision; No malignant transformations or metastasis |